
Page 31 - ISAKOS 2019 Newsletter Vol II
P. 31
02A Force-controlled compartment-specific
ligament tensioner.
CURRENT CONCEPTS
01 Illustrations of the knee in extension (left) and flexion (right).
The red line shows the level of tibial bone resection. When the bone is resected to the thickness of the implant on both the arthritic (medial) and intact (lateral) sides, the joint line on the medial side rises by 2 – 3 mm from the original (pre-arthritic) joint line. As the wear of bone and cartilage usually occurs on the medial aspect of the distal part of
the femur and not at the posterior aspect of the medial condyle, the elevation of the medial joint line can cause a tight medial flexion gap unless the PCL is resected. The double-headed red arrow represents the width of bone resection at lateral side. The blue rectangular area represents the tibial implant. The dotted line represents the original (pre-arthritic) medial joint line. The single-headed red arrow represents the elevation of the medial joint line. TEA = transepicondylar axis.
In principle, the bone resection level on the distal part of the femur is set so that the thickness of the medial side is equal to that of the implant. Because most varus knees have bone and cartilage wear on the medial side of the distal part of the femur, the medial joint line of the distal part of the femur is raised by 2–3 mm to be at the same level as the lateral side (Fig. 3). In cases in which the medial flexion gap is still larger than the extension gap, the resection level can be set more proximally in order to adjust the gap balance. However, because excessive elevation of the joint line will cause mid-flexion instability, gap differences can be adjusted by resection of the posterior part of the medial femoral condyle. After resection of the distal part of the femur, the extension gap can be assessed with the ligament tensioner or spacer blocks of the same thicknesses as the femoral and tibial components.
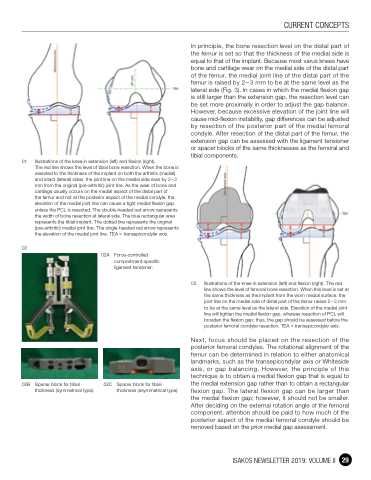
03 Illustrations of the knee in extension (left) and flexion (right). The red line shows the level of femoral bone resection. When this level is set at the same thickness as the implant from the worn medial surface, the joint line on the medial side of distal part of the femur raises 2 – 3 mm to be at the same level as the lateral side. Elevation of the medial joint line will tighten the medial flexion gap, whereas resection of PCL will broaden the flexion gap; thus, the gap should be assessed before the posterior femoral condylar resection. TEA = transepicondylar axis.
Next, focus should be placed on the resection of the posterior femoral condyles. The rotational alignment of the femur can be determined in relation to either anatomical landmarks, such as the transepicondylar axis or Whiteside axis, or gap balancing. However, the principle of this technique is to obtain a medial flexion gap that is equal to the medial extension gap rather than to obtain a rectangular flexion gap. The lateral flexion gap can be larger than the medial flexion gap; however, it should not be smaller. After deciding on the external rotation angle of the femoral component, attention should be paid to how much of the posterior aspect of the medial femoral condyle should be removed based on the prior medial gap assessment.
02
02B Spacer block for tibial thickness (symmetrical type).
02C Spacer block for tibial thickness (asymmetrical type).
ISAKOS NEWSLETTER 2019: VOLUME II 29
