
Page 18 - ISAKOS 2021 Newsletter Volume 1
P. 18
CURRENT CONCEPTS
The Eeklo Subvastus Approach for Total Knee Arthroplasty Detailed Surgical Technique
The VMO is lifted to check its distal attachment to the patella, linked to the superior edge of the easily recognizable medial patellofemoral ligament (MPFL) (Fig 3).
The cut is extended distally. Blunt forceps are inserted and are slid distally between the retinaculum and the underlying periosteum down to resistance, which is created by the attachment of the pes anserinus. The retinaculum is transected, with care being taken not to damage the subcutaneous fat, which can be gently manually peeled. The medial tissue contains the infrapatellar branch of the saphenous nerve.
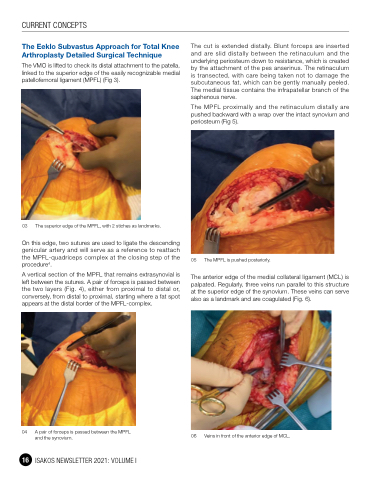
The MPFL proximally and the retinaculum distally are pushed backward with a wrap over the intact synovium and periosteum (Fig 5).
05 The MPFL is pushed posteriorly.
The anterior edge of the medial collateral ligament (MCL) is palpated. Regularly, three veins run parallel to this structure at the superior edge of the synovium. These veins can serve also as a landmark and are coagulated (Fig. 6).
06 Veins in front of the anterior edge of MCL.
03 The superior edge of the MPFL, with 2 stiches as landmarks.
On this edge, two sutures are used to ligate the descending genicular artery and will serve as a reference to reattach the MPFL-quadriceps complex at the closing step of the procedure4.
A vertical section of the MPFL that remains extrasynovial is left between the sutures. A pair of forceps is passed between the two layers (Fig. 4), either from proximal to distal or, conversely, from distal to proximal, starting where a fat spot appears at the distal border of the MPFL-complex.
04 A pair of forceps is passed between the MPFL and the synovium.
16 ISAKOS NEWSLETTER 2021: VOLUME I
