
Page 41 - ISAKOS 2018 Newsletter Volume 2
P. 41
Critical Shoulder Angle and Impact on RTC Repair
Francesco Franceschi, MD, PhD
Campus Biomedico University of Rome Rome, ITALY
The purpose of rotator cuff repair is to facilitate healing of the tendon within the native site. In many studies, surgical repair has been associated with success rates of 85% to 90%, with good clinical results. However, retears may occur, especially in older patients with large tears. Several studies have shown that rotator cuff re-tears after surgery depend on biomechanical, biochemical, and physiological factors that, together with additional unknown local factors, regulate the tendon-regeneration process. The process of connective-tissue repair seems to resemble that of wound- healing, although the details of the regulatory mechanisms remain unclear.
The rate of recurrence following surgical treatment ranges from 13% to 94% and is related to the quantity and quality of tendon tissue, age, and other factors. To decrease this rate, surgeons have sought to improve the surgical techniques and materials used. Biological factors (e.g., platelet-rich plasma [PRP]) and increasingly personalized rehabilitation programs, either delayed or accelerated, also have been used in an attempt to promote healing of the area, but the results have been poor.
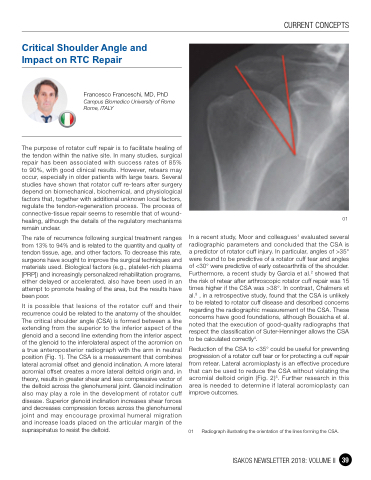
It is possible that lesions of the rotator cuff and their recurrence could be related to the anatomy of the shoulder. The critical shoulder angle (CSA) is formed between a line extending from the superior to the inferior aspect of the glenoid and a second line extending from the inferior aspect of the glenoid to the inferolateral aspect of the acromion on a true anteroposterior radiograph with the arm in neutral position (Fig. 1). The CSA is a measurement that combines lateral acromial offset and glenoid inclination. A more lateral acromial offset creates a more lateral deltoid origin and, in theory, results in greater shear and less compressive vector of the deltoid across the glenohumeral joint. Glenoid inclination also may play a role in the development of rotator cuff disease. Superior glenoid inclination increases shear forces and decreases compression forces across the glenohumeral joint and may encourage proximal humeral migration and increase loads placed on the articular margin of the supraspinatus to resist the deltoid.
01
In a recent study, Moor and colleagues1 evaluated several radiographic parameters and concluded that the CSA is a predictor of rotator cuff injury. In particular, angles of >35° were found to be predictive of a rotator cuff tear and angles of <30° were predictive of early osteoarthritis of the shoulder. Furthermore, a recent study by Garcia et al.2 showed that the risk of retear after arthroscopic rotator cuff repair was 15 times higher if the CSA was >38°. In contrast, Chalmers et al.3 , in a retrospective study, found that the CSA is unlikely to be related to rotator cuff disease and described concerns regarding the radiographic measurement of the CSA. These concerns have good foundations, although Bouaicha et al. noted that the execution of good-quality radiographs that respect the classification of Suter-Henninger allows the CSA to be calculated correctly4.
Reduction of the CSA to <35° could be useful for preventing progression of a rotator cuff tear or for protecting a cuff repair from retear. Lateral acromioplasty is an effective procedure that can be used to reduce the CSA without violating the acromial deltoid origin (Fig. 2)5. Further research in this area is needed to determine if lateral acromioplasty can improve outcomes.
01 Radiograph illustrating the orientation of the lines forming the CSA.
CURRENT CONCEPTS
ISAKOS NEWSLETTER 2018: VOLUME II 39
